Technological production to support the management of Basic Health Units: primary Health Care management software
Produção tecnológica de apoio à gestão de Unidades Básicas de Saúde: software de gestão de Atenção Primária à Saúde
Producción tecnológica de apoyo a la gestión de las Unidades Básicas de Salud: software de gestión de Atención Primaria
DOI: 10.59681/2175-4411.v17.2025.1115
Takanori Ogawa
Universidade Federal de Santa Catarina
https://orcid.org/0009-0009-4408-2742
Fernanda Paese
Universidade Federal de Santa Catarina
https://orcid.org/0000-0002-9672-4446
Deniz Faccin
Prefeitura Municipal de Florianópolis
Greici Capellari Fabrizzio
Universidade Federal de Santa Catarina
https://orcid.org/0000-0002-3848-5694
Daniela Couto Carvalho Barra
Universidade Federal de Santa Catarina
https://orcid.org/0000-0003-4560-7706
Gabriela Marcellino de Melo Lanzoni
Universidade Federal de Santa Catarina
https://orcid.org/0000-0001-5935-8849
Autor Correspondente: Greici Capellari Fabrizzio
Artigo recebido: 31/07/2023 | Aprovado: 21/11/2024
ABSTRACT
Objective: to present the development and evaluate the use of a software for the management of basic health units, with emphasis on material resources, infrastructure, personnel management and strategic planning. Methods: technological production from the development and usability stages of the PHC Management Software. The Unified Modeling Language and Rational Unified Process models were used for development, and the International Organization for Standardization standard for usability was used for quality and usability analysis. Results: Based on the needs identified together with the stakeholders, the software was developed in the following modules: human resources management; Basic Health Units; programs and actions, as well as process mapping. The software's usability test achieved an average score of between 3.6 and 4.5. Conclusion: The technological production developed has the potential to optimize processes and standardize information for health management at the municipal level.
Descriptors: Health Management; Software; Primary Health Care.
RESUMO
Objetivo: apresentar o desenvolvimento e avaliar o uso de um software de gestão de unidades básicas de saúde, com ênfase em recursos materiais, infraestrutura, gestão de pessoal e planejamento estratégico. Métodos: produção tecnológica a partir das etapas de desenvolvimento e usabilidade do Software Gestão APS. Para o desenvolvimento utilizou-se os modelos da modelagem Unified Modeling Language e do processo Rational Unified Process e para análise da qualidade e usabilidade utilizou-se o padrão da Organização Internacional para Padronização para usabilidade. Resultados: Baseado nas necessidades identificadas em conjunto com os stakeholders, o desenvolvimento do software pautou-se nos seguintes módulos: gestão de recursos humanos; de Unidades Básicas de Saúde; de programas e ações, além de mapeamento de processos. O teste de usabilidade do software alcançou a média entre 3,6 a 4,5. Conclusão: A produção tecnológica desenvolvida tem potencial de otimizar processos e padronizar informações para gestão em saúde a nível municipal.
Descritores: Gestão em Saúde; Software; Atenção Primária à Saúde.
RESUMEN
Objetivo: presentar el desarrollo y evaluar el uso de un software para la gestión de unidades básicas de salud, con énfasis en recursos materiales, infraestructura, gestión de personal y planificación estratégica. Método: producción tecnológica de las etapas de desarrollo y usabilidad del Software de Gestión de la APS. Para el desarrollo se utilizaron los modelos Unified Modeling Language y Rational Unified Process, y para el análisis de calidad y usabilidad, el estándar de usabilidad de la Organización Internacional de Normalización. Resultados: A partir de las necesidades identificadas con las partes interesadas, el software se desarrolló en los siguientes módulos: gestión de recursos humanos; Unidades Básicas de Salud; programas y acciones, así como mapeo de procesos. La prueba de usabilidad del software obtuvo una puntuación média de entre 3,6 y 4,5. Conclusión: La producción tecnológica desarrollada tiene potencial para optimizar los procesos y estandarizar la información para la gestión de la salud a nivel municipal.
Descriptores: Gestión en Salud; Programas Informáticos; Atención Primaria de Salud.
INTRODUCTION
Primary Health Care (PHC) in Brazil, the main gateway for people to enter the Unified Health System (SUS), is characterized by the organization of services into a network based on structuring elements: access at first contact, comprehensiveness, longitudinally, coordination of care, family and community orientation and cultural competence. Responsible for coordinating healthcare, PHC requires managers and providers capable of guaranteeing qualified access, considering the challenges of equalizing material and human resources in the face of growing demand and health crises at local or regional level(1).
Planning and organization must be based on recognition of the regional reality. It is necessary to identify the most pertinent planning tools for developing networks to make the best use of existing resources in each territory, considering the quantitative correspondence to the assigned population contingent and its specificities, which are fundamental elements for organizing work processes and user health care(2-3).
Structural deficiencies in health units and the lack of supplies and equipment have an impact on the dissatisfaction of family health team professionals(3). In addition, the lack or high turnover of health professionals has a significant impact on care practices, weakening the bond with the community, understanding of flows and micro-regulatory processes in the health care network(2).
Although public spending on health in Brazil is relatively lower than in countries with health systems with similar characteristics, from the point of view of efficiency, there is potential for improvement in PHC, which was 68% efficient in 2017. Among the possibilities for efficiency gains were the training of health professionals to manage health information(4). In this sense, there is a shortage of professionals trained to work with and analyze information databases, resulting in low commitment and accountability in the implementation of team-based health planning(5-6).
Another aspect of efficiency gains is the introduction of technologies and incentives to increase professional productivity. Information and communication technology (ICT) in the health sector has expanded greatly in recent years. In the latest Health at a Glance report (2021), there was a significant digital expansion in health in OECD countries during the covid-19 pandemic, in which 45% of adults had a medical teleconsultation in 2021(7). In addition, around 60 per cent of adults searched for health information online in 2020, up from 36 per cent in 2010(7). Regarding management, contemporary approaches emphasize that the use of ICTs increases access to information, contributing to increased transparency, assertiveness in decision-making, improved accountability and the fight against fraud and inconsistencies. These aspects allow for better use of resources, which makes the service more efficient and financially sustainable(8).
In this sense, considering the potential of using information technologies to support management, the aim of this study was to present the development and evaluate the use of software to manage basic health units, with an emphasis on material resources, infrastructure, people and planning.
METHODOLOGY
The APS Management Software technological production method was divided into two stages, the first covering the software development stages and the second usability. Software development used sections of the iterative software development model and processes to minimize errors in software design, using the Unified Modelling Language (UML) modelling stages and the Rational Unified Process (RUP)(9-10).
The software's quality and usability analysis used the International Organization for Standardization (ISO) standard and the ISO/IEC 25010 and NBR ISO 9241-11 standards, thereby verifying user acceptance(11).
SOFTWARE DEVELOPMENT
The stages of the development process are shown in Table 1. The flow of the stages was guided by the RUP sections: initiation, elaboration, construction and transition. Good practices were used, such as developing iteratively and managing the requirements, changes and improvements requested by the stakeholders. In this context, stakeholders are key people in the development of the activities, such as health professionals, managers, information and communication technology professionals, among others(12).
Table 1: Stages of the APS Management Software development processes
|
Stages of Technological Production |
Software development |
|
|
1 |
Outline phase |
Definition of the software's scope, purpose and stakeholders. |
|
2 |
Gathering of requirements |
Sequence of activities and brainstorming with stakeholders. |
|
3 |
Requirements Analysis |
Refining the requirements gathered and analyzed. |
|
4 |
Programming tools |
Choice of infrastructure with computational scalability architecture. |
|
5 |
Creating a Database |
Database modelling. |
|
6 |
Documentation |
Documentation with diagrams and flows. |
|
7 |
Development |
Translation of requirements into programming language. |
|
8 |
Prototyping |
Refining visual models. |
|
9 |
Creating the Interface |
Acceptance of the stakeholder environment. |
|
10 |
Testing |
Verification of the software's usability with stakeholders. |
|
11 |
Implementation |
Provision of a computing environment for users. |
Source: the authors (2022)
The software development team was made up of four people with multidisciplinary skills: a developer and three stakeholders who are specialists in Health Management, one of whom is a dentist and a nurse from the municipality's Health Department, and a lecturer linked to the Postgraduate Program in Health Informatics.
The software development process using an incremental and iterative approach facilitated the design of the software, as the product was adapted to accept the changes requested by the users, and to be closer to the requirements requested at the start of development by the stakeholders.
The software was developed using the PHP, CSS and JavaScript programming languages, along with the Bootstrap framework. This set of technologies was chosen to improve the quality of the graphical interface, ensure agility in development and make programming more dynamic. For data storage, we used MySQL Server, an open-source relational database. The backup routine was manual, and the backup files were saved in the institutional OneDrive cloud at the Federal University of Santa Catarina.
The choice of development tools was based on their ability to integrate with other languages, their scalability, popularity and the high level of documentation available on the internet. The infrastructure used for development was of the client-server type, using virtualized web and database servers to access the development module files.
Usability evaluation
The research site was the Health Department of a municipality of approximately 500,000 inhabitants that uses its own electronic health record system. Because it uses its own system, the data collected in the health services must be exported to the federal SUS systems, increasing rework and duplication of information. The SUS systems and the one used in the municipality do not yet fully meet some of the functionalities for managing material resources, infrastructure, people and planning, which is why a Health Management system is needed, which justifies the objective and choice of scenario for this research.
The selection of users for the usability test was intentional and non-probabilistic. For the pilot test, 10 per cent of the population was randomly selected. This percentage made it possible to test the software and assess the feasibility of the research, indicating weaknesses and problems in the software and making it possible to resolve the faults before implementation. Initially, five managers were randomly selected to take part in the pilot test. Of the five managers, one was unable to take part because he was on holiday.
To carry out this final study, 47 professionals working in management and coordination positions in the Basic Health Units (BHUs) of the municipality's Health Department were invited. Participants from the health sector were selected because of their experience in health management and their potential for analyzing performance, errors and software quality. Out of a total of 52 participants included in the study, 30 professionals responded. The reasons for not taking part were holidays, time off work and work overload related to the COVID-19 pandemic.
The research was conducted in a municipality with four Health Districts, which are decentralized PHC management sectors. Initially, the pilot test was carried out in the Centre Health District, randomly selecting managers. This approach made it possible to test the software and assess the feasibility of the research, with the aim of identifying possible weaknesses and problems in the software. The aim was to resolve any flaws before implementation. After final adjustments to the collection instrument, the usability test was applied to the other professionals in the other Health Districts.
Data collection covered the period from 4 June to 31 July 2021 and the survey instrument focused on user acceptance of the Gestão APS software, analysis of the suitability of the management functionalities, user satisfaction with the system and, above all, the execution of tasks electronically with the tool. The usability evaluation criteria included ease of use, productivity, memorization, protection against errors and the software's adherence to the management work of the BHUs.
The users analyzed the usability requirements of the ‘Gestão APS’ software considering: Meeting the needs of PHC management practice; Systematization of information records, with easy updating and reducing excessive rework; BHU-specific information; Technology portability; Easy user access; The monitoring of strategic actions and programs.
The usability measurement criteria were broken down according to ISO 9241 definitions, in which the user achieved the usability, effectiveness, efficiency, satisfaction and interface objectives of the BHU Health Management software(10). The studies were centered on descriptive statistics involving calculations of absolute frequency, central tendency (mean), standard deviation and data analysis/interpretation using inferential statistics. Usability consisted of evaluating the interface in terms of user experience. It has a 5-point scale format (1 - Strongly disagree, 2 - Partially disagree, 3 - Neither agree nor disagree, 4 - Partially agree, 5 - Strongly agree). The evaluation considered mean values between 1 and 2.50 ‘Negative Positioning’; from 2.51 to 3.5 ‘Neutral Positioning’; from 3.51 to 5.0 ‘Positive Positioning’(11-10).
The data collection instrument was structured in digital forms, implementing data security and preservation measures, guaranteeing confidentiality, integrity, authenticity and availability. All the guidelines of the General Data Protection Act were strictly followed to ensure compliance. To preserve the privacy of the participants, a code was assigned, consisting of the letter P, followed by a cardinal number (1,2,3...30) corresponding to the order in which the completed online form was submitted. Participants were informed about the risks and benefits of the research, clarifying and raising awareness of the importance of the nature and construction of scientific knowledge. The research was submitted to the UFSC Human Research Ethics Committee, and the report number is 39908820.6.008.0121.
RESULTS
The software was developed with a focus on healthcare management needs and stakeholder requirements. The development process included stages of initiation, elaboration, construction and transition. In the initiation stage, requirements were gathered. In the elaboration stage, the requirements were analyzed, and the database was created. The construction stage involved software documentation and prototyping. Finally, in the transition stage, the interface was created, usability tests were carried out and the software was deployed. All the stages were essential to ensure that users' needs were properly met and that the software was of high quality throughout the development process.
Table 2 shows the initial requirements raised/identified and the functionalities implemented and developed in the “Gestão APS” software. By characterizing the needs of health managers, it was possible to visualize the requirements needed to develop the correct functionalities for the software without losing the final purpose of creating software that adheres to health management.
Table 2 - Presentation of modules, identified needs and functionalities implemented
|
# |
Module |
Identified Needs |
Functionality/ Implementation |
|
1 |
HR Management |
- Register information on healthcare professionals. - Centralized and standardized information. |
Classify and monitor information from health professionals. |
|
2 |
BHU management |
- Register BHU information. - Centralized and standardized information. |
Classifying and Monitoring BHUs |
|
3 |
Action and Program Management |
-Register BHU Structure and Equipment. - Information on BHU structures and equipment. |
List of services available at BHUs. |
|
4 |
Process Mapping |
- Standardization of information on Professionals, Teams, Structure and Equipment and Visualization of information in Reports. - Retrieve information from BHUs and Professionals. |
Monitor and map BHU information. |
Figure 1 shows the importance of stakeholders in the software prototyping phase, as visual elements were incorporated as a banner to make the screen more pleasant, showing the versions of the development, which was centered on the needs of the end user.
 First, second, third and definitive draft. Source: the authors (2022)
First, second, third and definitive draft. Source: the authors (2022)
Figure 1 - Team screen - from prototyping to defining the final screen.
The requirements survey asked for a screen to control BHU workers, in which managers could have visual control of each employee's working hours. Figure 2 shows the colors according to each worker's situation: red indicates long-term sick leave, yellow partial sick leave and green normal sick leave. The numbers indicate the number of hours each employee works per week: 20, 30 or 40 hours.
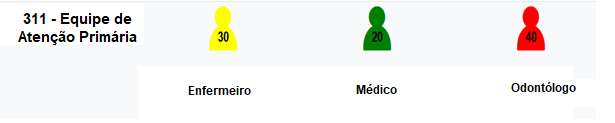
311 – Primary care team: (30) nurse, (20) doctor and (40) dentist. Source: the authors (2022)
Figure 2 - Screen where the BHU manager controls the worker's working hours.
The refinement of the requirements and changes to the software were carried out with constant consultation and approval from the development team, who were the main partners in the software's development. Frequent communication with stakeholders made it possible to minimize implementation failures and improved the quality of the final product's usability, promoting ease of use and learning. Table 3 shows the averages and standard deviation of the criteria evaluated by the participants.
Table 3 - Usability Criteria for APS Management Software
|
Usability criteria |
Average |
SD |
|
1. Software Content Criteria |
4,07 |
0,522 |
|
2. Effectiveness Criteria |
4,34 |
0,199 |
|
3. Efficiency Criteria |
3,60 |
0,216 |
|
4. Satisfaction Criteria |
4,20 |
0,041 |
|
5. Interface criteria |
4,50 |
0,036 |
Source: the authors (2022)
In the study carried out, the software received positive evaluations in different criteria. In terms of usability, the evaluators were positive, with an overall average of 4.07. This indicates that the software was considered easy to use and intuitive by users. As for effectiveness, the software obtained an overall average of 4.34, which shows that it was considered effective for carrying out management tasks in BHUs. Although the scores were high in this criterion, it is worth mentioning that there were requests to implement new features. In terms of efficiency, the software had an overall average of 3.6, with a percentage of affirmations between neutral and positive. This indicates that, in the short period of use, the software may not have had a positive impact on optimizing health management processes in the BHUs. However, it is important to consider that the participants left comments that confirm this result.
User satisfaction with the software was significant, with an overall average of 4.2. This means that the participants felt comfortable using the software, showing good receptivity and acceptance. In terms of the interface, the software's design received an overall average of 4.5, indicating that it was considered pleasant by the users. The overall results show that the software was well evaluated by users in terms of usability, effectiveness, satisfaction and interface, reflecting a positive reception in different aspects of the health management software in BHUs.
DISCUSSION
The software was developed to support the management of Basic Health Units, which are part of Primary Health Care. Although this part of the Health Care Network is not characterized by high-density technological resources like the secondary (complex specialties and medical exams) and tertiary (hospitals) levels, the management of BHUs involves a complex work process that includes human relations between managers, the community, users and the team, with the challenges of intangibility, the difficulty of standardization, the importance of the human factor, the simultaneity between production and consumption, the impossibility of stockpiling, among others(13).
The complexity of health management processes and the challenge of encompassing the different needs of PHC professionals were minimized by the iterative development model, facilitating the process of characterizing the health management requirements of the BHUs in the municipality studied. The development tool made it possible to properly incorporate health management functionalities into the software, minimizing errors in the development phase and helping to detect errors in many stages of the software's development.
The software was developed in the form of four modules related to BHU management: HR management, BHU management, action and program management and process mapping. Some of the functionalities provided in the modules can be seen to contribute to the work process of BHU managers.
For example, one of the challenges faced by managers is the high turnover of health professionals in PHC, which compromises continuity of care, the creation of bonds and coverage of territories(14). It's important to highlight the main functionalities of health management software in BHUs. The PHC Management software allows managers to view the status of each health professional, indicating whether they are currently active or on leave. The functionality helps organize work, allowing for more efficient planning based on the availability of professionals. The PHC Management software makes it possible to identify the need to reorganize or request new health professionals, with the aim of optimizing the distribution of resources and guaranteeing an adequate team to meet the health demands of the BHUs. This increases visualization and planning capacity, contributing to more effective and assertive management and improving the quality of the services provided.
The composition of a multidisciplinary development team was fundamental to reducing errors in requirements and functionalities, increasing reliability and integrity, as well as making the software as scalable as possible. By adding the experiences and needs of users/health professionals, the project was guided in the development phase and in improving the technological solutions already developed(15).
Stakeholders played an important role in the software development process, as their knowledge and experience of healthcare management was essential in gathering requirements and prototyping, simplifying the software development process. The high averages in the usability criteria show that the minimalist design did not compromise users' ability to carry out tasks in the software.
The purpose of software development with the participation of stakeholders is to show the research participants that health professionals were involved from the conception, planning, implementation, support and dissemination of the software's usability results, strengthening the purpose and objective of the development(12). A successful software development project is linked to how the client receives the project, so the constant interaction between the parties involved in the project directly influences its success(16).
The pilot test carried out, in which users could interact with the software and test its usability, made it possible to detect and identify usability problems, thereby aligning the software's requirements and features. The pilot helped to engage end users and users of the software.
The usability test involving users enabled them to report errors that appeared in the software and to measure them through positive and negative comments as the test progressed(17-18). The questionnaire was carried out on an online form, with no moderation by an interviewer, making it difficult for the developer and users to interact. On the other hand, with the virtual form, users were free to express their opinions and suggestions about the software without the pressure of an interviewer trying to induce the user to respond positively.
The software's usability test averaged between 3.6 and 4.5 among the participants who evaluated the software, thus showing that there were minor usability errors identified by the participating users. The use of averages to analyze the values is less biased and reduces the possibility that the result is not so divergent from the opinion of the participants(19). The level of learning evaluated in the efficiency and effectiveness criteria reached an average of between 3.6 and 4.34, which shows that they had a low evaluation due to the participants' lack of experience in using the software, i.e. the short time the users had been testing the software, which meant they didn't have time to get used to using it(19). To try to mitigate the problems reported by users, stakeholders were informed about design and requirements problems, thereby helping to improve usability.
The usability rating by the participants showed that the standardization of information and the centralization of data can be positive for health management. The result of the favorable usability evaluation shows that the software is on the right track to try to solve the deficiency in health management technology and, above all, to be a tool for innovation in the development of management and communication technologies.
CONCLUSION
The COVID-19 pandemic has made face-to-face interaction with the user in the test environment difficult, and many mediations have used remote technologies to provide training and support to the user, often requiring inadequate infrastructure and the patience and flexibility of everyone involved in the software development and testing process.
Primary care management is complex and has a number of particularities, which are not covered by official systems or even those contracted by municipalities through tenders, since in this case the functionalities need to be described and there is no flexibility to develop a more personalized product with iterative development. Technological production can be a way of improving processes and standardizing information for health management at local/municipal level. However, the implementation of new technologies is still a challenge regardless of the area.
This model proved to be positive because it made it possible to develop a technological product with a high level of customization and adaptation to the needs of PHC management. In this way, this model achieved the expected objective by presenting the development and evaluating the use of a software program for managing basic health units, with an emphasis on material resources, infrastructure, people and planning.
The meetings with the stakeholders minimized and facilitated the coding work in programming language, because the Health Management information was presented correctly and clearly to the developer. The decision to build the design together with the stakeholders proved to be effective, supported by the high interface averages of 4.2 and 4.5 in the survey. The stakeholders' knowledge of BHU health management was fundamental to presenting software that met the needs of BHU coordinators.
One limitation is that the software did not incorporate accessibility features, such as high contrast and font size control. The challenge in future versions will be to integrate the necessary resources to increase accessibility, as well as integration with other information systems.
REFERENCES
1. Giovanella L, Mendonza-Ruiz A, Pilar A de CA, da Rosa MC, Martins GB, Santos IS, et al. Sistema universal de saúde e cobertura universal: desvendando pressupostos e estratégias. Ciênc. saúde colet. 2018;23:1763–1776.
2. Almeira PT, Silva KS, Bousquat A. Atenção Especializada e transporte sanitário na perspectiva de integração às Redes de Atenção à Saúde. Ciênc. saúde colet. 2022;27:4025–4038.
3. Moreira KS, Lima C de A, Vieira MA, Costa S de M. Avaliação da infraestrutura das unidades de saúde da famı́lia e equipamentos para ações na atenção básica. Cogit. Enferm. 2017;22(2):1-10.
4. Araujo EC, Lobo MSC, Medici AC. Eficiência e sustentabilidade do gasto público em saúde no Brasil. J Bras Econ Saúde. 2022:14(1):86–95.
5. Ferreira J, Celuppi IC, Baseggio L, Geremia DS, Madureira VSF, de Souza JB. Planejamento regional dos serviços de saúde: o que dizem os gestores? Saúde Soc. 2018:27(1):69–79.
6. Pinheiro ALS, Andrade KTS, Silva D de O, Zacharias FCM, Gomide MFS, Pinto IC. Health management: the use of information systems and knowledge sharing for the decision making process. Texto contexto-enferm. 2016:25(3);e3440015.
7. Organisation for Economic Co-operation and Developmente - OECD. Executive summnary in Health at a Glance. 2021 [citado 2022 jun 02]. Disponível em: https://www.oecd-ilibrary.org/content/component/d7b43a94-en
8. Matos AA, Nunes AM. Tecnologias da informação e comunicação no sistema de saúde Português. J. Health Inform. 2018:10(1):30-4.
9. Sommerville I. Engenharia de software: uma abordagem profissional. 8a. edição. Porto Alegre: AMGH; 2016.
10. International Organization for Standardization - ISO/IEC 25010:2011. Systems and software engineering – Systems and software Quality Requirements and Evaluation (SQuaRE)– System and software quality models. 2011 [citado 2022 jun 02]. Disponível em: https://www.iso.org/standard/35733.html
11. Associação Brasileira de Normas Técnicas - ABNT. NBR 9241-11 Requisitos ergonômicos para trabalho de escritório com computadores: Parte 11—Orientação sobre usabilidade. 2021. [citado 2022 jun 02]. Disponível em: https://www.inf.ufsc.br/~edla.ramos/ine5624/_Walter/Normas/Parte%2011/iso9241-11F2.pdf
12. Norris JM, White DE, Nowell L, Mrklas K, Stelfoc HT. How do stakeholders from multiple hierarchical levels of a large provincial health system define engagement? A qualitative study. Implementation Science. 2017:12;1–13.
13. Pires DEP de, Vandresen L, Machado F, Machado RR, Amadigi FR. Primary healthcare management: What is discussed in the literatura. Texto contexto - enferm. 2019;28: e20160426.
14. Tonelli BQ, Leal APR, Tonelli WFQ, Veloso DCM, Gonçalves DP, Tonelli SQ. Rotatividade de profissionais da Estratégia Saúde da Famı́lia no municı́pio de Montes Claros, Minas Gerais, Brasil. RFO UPF. 2018:23(2):180-185.
15. Gonçalves LS, Amaro MLM, Romero ALM, Schamne FK, Fressatto JL, Bezerra CW. Implementation of na Artificial Intelligence Algorithm for sepsis detection. Rev Bras Enferm. 2020;73(3):e20180421.
16. Tam C, Moura EJ da C, Oliveira T, Varajão. The factors influencing the success of on-going agile software development projects. International Journal of Project Management. 2020;3:165-176.
17. Nielsen J. usability heuristics for user interface design. Nielsen Norman Group. 1994:8;2021.
18. Nielsen J, Molich R. Heuristic evaluation of user interfaces. Proceedings of the SIGCHI conference on Human factors in computing systems. 1990;249–256.
19. Tullis T, Albert B. Measuring the user experience: Collecting, Analyzing and Presenting Usability Metrics. 2a ed. Morgan Kaufmann; 2013.
Como Citar
Ogawa T, Paese F, Faccin D, Fabrizzio GC, Barra DCC, Lanzoni GM de M. Produção tecnológica de apoio à gestão de Unidades Básicas de Saúde: software de gestão de Atenção Primária à Saúde. J Health Inform [Internet]. 3º de janeiro de 2025 [citado 14º de março de 2025];17(1):1115. Disponível em: https://jhi.sbis.org.br/index.php/jhi-sbis/article/view/1115
Licença
 Este trabalho está licenciado sob uma licença Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Este trabalho está licenciado sob uma licença Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.